Photo-Illustration: Viktor Koen
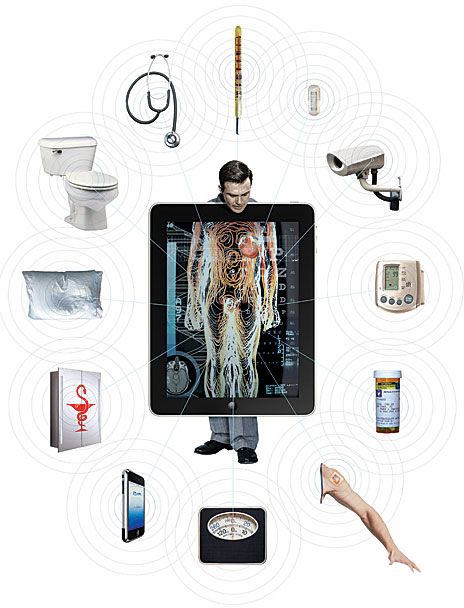
Imagine a world in which your medicine cabinet notices that you are due for a prescription refill and calls it in. A sensor implanted under your skin detects a fluid buildup in your lungs and alerts your doctor, who decides your heart medication needs an adjustment and contacts the pharmacist to change your dosage. Meanwhile, sensors in your toilet confirm that your body has adjusted well to your other medications but sees indications that you may be a borderline diabetic. Your doctor, given these readings and your family medical history, suggests that you change your diet. Noting that fact, your bathroom scale asks you to punch in a weight-loss goal and starts giving you a regular progress update. Your medical checkup isn’t an annual event—it happens every day, simply as you go about your daily life.
If such ambient monitoring and intervention strikes you as a little creepy, think of it this way: It could avert a heart attack, stroke, or other medical crisis. It could keep you out of the hospital and save money for both you and the health care system. Part of the savings would come from radical changes in the management of chronic diseases, which in the United States eats up 75 percent of health care spending, or about US $1.9 trillion each year.
And a health-monitoring bathroom is not science fiction. This is what health care could look like within the decade, at least for some. Perhaps predicting such dramatic change within 10 years is overly optimistic. But the necessary technologies already exist or are close at hand, the need to reduce health care costs is real, and the current health care system demands change. What’s more, a groundswell of support for wireless health care is rising from a diverse group of people and organizations. These include communities of consumers who want better ways to manage and measure their own health, like the Quantified Self movement andHealth 2.0, which sponsors competitions to spur the development of new health care apps and devices. Also on board are nonprofit organizations like the West Wireless Health Institute, in La Jolla, Calif., where I work as chief medical and science officer. We focus on lowering health care costs through health technology innovation. The nonprofit LeadingAge Center for Aging Services Technologies is working to improve quality of life for the aging. For the third year in a row, the U.S. National Institutes of Health is hosting the global mHealth Summit, a conference examining the impact of mobile technologies on health care delivery, research, business, and policy. And hundreds of start-ups are exploring near-term and long-term ways to reform the delivery of health care.
Change is happening. Yes, a technological revolution in health care has been predicted before, but we are at an inflection point now, where wireless connectivity, personal cellular devices, pervasive sensing technologies, social networks, and data analytics are mature enough to make wireless medicine a reality. And there is a will as never before to find a way to reduce crippling health care costs. Already, new devices allow diseases like diabetes and chronic heart failure to be closely monitored outside the doctor’s office; tools for tracking chronic kidney disease and a variety of lung disorders are sure to follow. Eventually, most health care will occur not during occasional visits to doctors’ offices, clinics, or hospitals but continuously, during ordinary activities in people’s homes, cars, and workplaces.
A trial program by the U.S. Department of Veterans Affairs offered an early look at what systemic change could mean. In 2003, the VA began using simple messaging devices and occasional videoconferences to let chronically ill veterans stay in touch with nurses and other health care professionals. Under this program, one of the largest of its kind in the world, 71 000 veterans are now receiving daily monitoring for such conditions as diabetes, heart disease, and post-traumatic stress disorder.
The VA’s program involves veterans who typically have multiple chronic illnesses that could easily land them in the emergency room unless complications are caught early. In the initial pilot study, each patient was assigned a care coordinator and given a dedicated device—typically a gizmo from the German company Robert Bosch Healthcare called a Health Buddy, which is about the size of a landline telephone and has a small LCD screen with four large buttons to let the user keep in touch with the coordinator. The patient would regularly connect one or more vital-signs monitoring devices—a blood pressure cuff, for example, or a thermometer—to the Health Buddy and follow on-screen instructions to collect that data. The patient would also respond to questions on symptoms and behavior, such as, Have you taken your medicine? Are you feeling sad? This daily assessment was automatically uploaded to a secure server, and professionals managing the patient’s care then used a Web interface to look for problems. With this system, each care coordinator was able to monitor 125 patients, following up by videoconference as necessary.
The results have been striking. A December 2008 VA study of this program concluded that it had reduced hospital admissions by 19 percent and reduced days spent in hospitals or other health care facilities by 25 percent. At $1600 per patient per year, the telehealth program costs vastly less than visiting nurses ($13 121) or nursing home care ($77 745). It’s not just veterans who could benefit from such an approach. A January 2009 study by the New England Healthcare Institute estimated that use of this same technology for all U.S. patients at risk of heart failure—an estimated 1.27 million people—could save up to $6.4 billion annually through reduced hospital admissions.
As successful as it has been, the VA’s system is very simple telemedicine, in many cases using dial-up telephone connections and basic devices. Add today’s ubiquitous wireless connectivity and new mobile health-monitoring devices, and the benefits will be far greater.




If you’re one of the hundreds of millions of people in the world today with diabetes or heart disease, you could be among the first to experience the next phase of the wireless health care revolution. Wireless glucose monitors are already on the market from companies like Medtronic and DexCom, and the latest ones may soon be paired with insulin infusion pumps so they can automatically adjust insulin dosages in response to changes in the patient’s glucose level.
Most of the wireless glucose monitors consist of a patch containing a processor, a transmitter, and a thin platinum electrode that slips under the skin. The monitor samples blood glucose levels at fixed intervals—typically, every 5 minutes—calculates trends, and then passes that information to the infusion pump, which uses the data to calculate when and how much insulin to release. This kind of system allows far closer control of diabetes than a manual self-administered system, avoiding the need to prick the skin, collect a blood sample, insert that sample into a reader, and then pick the appropriate insulin dose. And supplying exactly the right amount of insulin just when it’s needed has been shown to prevent complications, including blindness, kidney disease, and peripheral vein disease that can lead to the loss of a limb.
People with congestive heart failure may soon benefit from a wireless monitor being developed byCardioMEMS. Its heart failure pressure-measurement system has two components: an implanted wireless sensor and an external electronics module. In the sensor device, a glass membrane shifts in response to pressure changes; the tiny movement changes the resonance frequency of an oscillating circuit in the sensor. The external module tracks these changes. This tracking method detects fluid buildup in the patient’s lungs, a common complication that often leads to hospitalization. The device can detect a problem even before the patient notices major symptoms; the doctor can then adjust the patient’s medication to reduce fluid levels.
Avoiding hospitalization is good for patients and for the health care system. The cost of a hospital stay in the United States for heart failure averages $10 000, and nearly 30 percent of those who are hospitalized will end up back in the hospital within 30 days. So provided the cost of the implant is kept reasonable, the potential savings from using it could be significant if it can avert even a single hospitalization.
Diabetes and heart disease are only the first of many conditions whose treatment will be improved by such monitoring tools. Down the road we’ll likely see similar approaches to blunt the progress of chronic kidney disease and prevent hospitalizations for chronic obstructive pulmonary disease, emphysema, and pneumonia, among other ailments.
But you’re reasonably healthy, you say, just a tad overweight and a bit too sedentary. Oh, and you should probably eat better. At least that’s what your doctor keeps telling you at every annual checkup. Maybe he suggests that you weigh yourself daily and log that information in a paper diary or an Excel spreadsheet. Maybe you even tried doing that but stopped after a few days.
Chances are your doctor didn’t suggest a more convenient way of monitoring your vital signs. Consider the $159 WiFi Body Scale, introduced two years ago by the French company Withings. It automatically uploads your weight and body-mass-index measurements to a secure website or mobile device and tracks trends in the data. You can view updates privately or send them to your doctor.
Or take a look at Panasonic’s wireless-enabled blood pressure monitor, also introduced two years ago. This $199 consumer device has a portable wireless display that saves up to 90 of an individual’s readings, which makes it easy to take to your next doctor’s visit. Similar to the Withings scale, this monitor makes it easy to track trends over time and allows doctors to note any changes that might require immediate intervention or those that should be discussed with the patient.
These two devices may not seem revolutionary; after all, they’re just standard products updated with telecommunications capabilities and Web interfaces. But they signal a sea change in health care. They enable physiological data, the basic vital signs collected routinely at the beginning of just about every visit to a doctor’s office, to be easily and automatically recorded and monitored over time.
Tracking such information is critical to effective health care; doctors know, for example, that having high blood pressure is less dangerous than having extreme fluctuations in blood pressure, and that a sudden weight increase can signal an imminent crisis for a heart patient. But without the right technology, tracking your vital signs isn’t easy, and the information may not reach your doctor in time to be meaningful.
These are just a few of the kinds of medical conditions and physical data that today can be monitored by sensors and wireless communications. Increasingly, people are turning to technology to gain a more complete picture of their overall health. In the past, the only way to obtain detailed information was through costly stays at high-end clinics or expensive medical tests. Now, however, it’s both affordable and widely available. Some of these monitoring systems are stand-alone devices, while others run on popular consumer gadgets like the iPhone or even through your car.
For example, for the many people who have trouble getting a good night’s rest—50 million in the United States alone—there are now a number of sleeping-aid devices either on the market or awaiting approval by the U.S. Food and Drug Administration or regulatory agencies in other countries. BiancaMed’s bedside sleep monitor is one of the most promising. About the size of an alarm clock, the SleepMinder uses motion sensors to measure your sleep quality, respiration, and any incidents of sleep apnea without having to make contact with your body. From these data, it creates a report that it sends to a website, where the user can print it out to take to a doctor for discussion. This process, which recently received FDA approval, could replace a costly stay in a sleep lab, which in the United States averages $2625. In addition to helping diagnose ordinary sleep disorders, it could also point to chronic conditions that affect sleep.
 Photo: Robert Bosch HealthcareBUDDY SYSTEM: Robert Bosch Healthcare’s Health Buddy automates remote patient monitoring.
Photo: Robert Bosch HealthcareBUDDY SYSTEM: Robert Bosch Healthcare’s Health Buddy automates remote patient monitoring.
A simpler device intended for consumer use is the Zeo Personal Sleep Coach, which is already available for $159. The Zeo system includes a headband with sensors that collect signals from the brain and eye and face muscles while the user moves from wakefulness into and out of deep and REM sleep. It doesn’t track respiration or apnea, though. The sensors transmit their data to a bedside device that graphs the information and gives each night’s rest an overall quality score.
If you suffer from irregular heartbeats or know somebody who does, a recently announced product from AliveCor may help. The company’s $100 case for the iPhone 4 enables the iPhone to run electrocardiograms (ECGs). If approved by the FDA, it would allow you to monitor heart rate and rhythm abnormalities, including atrial fibrillation, whenever you feel them occurring. That’s potentially a breakthrough, because patients who complain of heart rate irregularities don’t often experience them on cue. To use the AliveCor device, you press the iPhone in the special case against your bare chest or hold it in your hands. Silver electrodes on the back of the case detect the heart rate, which is then transmitted wirelessly via Bluetooth to the iPhone. An app translates the data into ECG graphs and turns them into PDFs.
Meanwhile, researchers at Georgia Tech have developed an iPhone app that assesses the tremors associated with Parkinson’s disease, potentially allowing doctors to better treat patients. The app, called iTrem, is beginning a clinical study at Emory University and will need FDA approval before it can hit the market.
Even Ford is getting into the wireless health care action. In May 2011, the company announced that it is developing in-car health tracking as part of its Sync system. Ford is working with companies like Medtronic that make instruments to measure blood glucose levels and software to help diabetic patients track their diet and medications. The first prototype system uses Bluetooth to connect the car to a continuous glucose-monitoring device. The system gives audio updates to the user and sounds an alarm if glucose levels fall too low, a situation that could lead to a loss of consciousness or a seizure—and be particularly dangerous on the road.
The United States isn’t the only country whose crippling health care costs and aging population are pushing the development of alternatives to traditional health care delivery; the same holds true in much of Europe and Japan. Conversely, in developing countries, where cellphones are as prevalent as almost anywhere else in the world, the United Nations Foundation and scores of nongovernmental organizations have been implementing mobile health (mHealth) programs, successfully reaching people who have little access to health care, with a focus on things like phoned¿in pill reminders for diseases such as tuberculosis, letting people know via text where they can find confidential HIV/AIDS testing, and using communications networks to track disease outbreaks and epidemics.
In some cases, the United States is behind the curve and must play catch-up. U.S. regulatory paths for approving new wireless medical devices remain unclear, although the FDA has been issuing draft guidance documents this summer and is working on the problem. The pervasive feeling in the industry, however, is that the United States is losing a competitive edge to Europe and other countries around the world. Kai Medical, for example, which makes a noncontact wireless device for continuous monitoring of respiratory rate, patterns, and activity, has already received the European Union’s certification of compliance (known as a CE) for its Kai Continuous device; U.S. approval for the same device is now pending.
Expanding wireless health care capabilities will lead in the coming years to what I call the “health-e-home.” This comprehensive health monitoring and treatment system will evolve from technology that today helps family members monitor aging relatives. For example, motion sensors installed in the home by companies like WellAware can track a resident’s daily activity levels. These sensing systems do far more than detect a sudden fall. They monitor ordinary tasks like getting out of bed, opening the refrigerator, and walking around the house and can spot any changes that can signal a problem. For instance, an elderly person who starts to sleep later each day, doesn’t leave home, and eats less frequently may be developing complications from medications, a worsening of congestive heart failure, or depression.
It’s not a big leap, then, to imagine augmenting such technology in a few years with a smart medicine cabinet, capable of tracking medications, warning about potential interactions, reordering prescriptions, and checking expiration dates. It could also interact with other devices, like the calendar on your smartphone (to remind you that you have an upcoming trip, so you’d better stock up on your prescriptions) or your refrigerator (to remind you not to drink grapefruit juice because you’re taking Lipitor). The benefits could be huge. The New England Healthcare Institute estimates that the cost of drug-related complications, including failure to take medications as directed, is as much as $290 billion annually—or 12 percent of total health care expenditures in the United States.
While a smart medicine cabinet can check that the right medicines are moving on and off the shelves as scheduled, it can’t tell if the patient is actually consuming them. In the future, wireless technology integrated into medications will be able to confirm that the patient has ingested the medicine. Proteus Biomedical, based in California, has developed digestible computer chips with built-in wireless transmitters. These ”ingestible event markers” are made from ingredients similar to those that bind vitamins into pills. Digestive fluids in the stomach activate the devices, which then create ultralow-power signals that can be picked up by a tiny recorder inserted under the skin or worn as a small adhesive skin patch. The recorder notes the date and time of the pill’s activation along with other information, such as the type of drug, dose, and place of manufacture. It also takes a snapshot of the patient’s heart rate, respiratory rate, and other physiological measurements. The detector then sends the information to a server that can combine it with data from other sensors, such as those that measure blood pressure, weight, and blood glucose, as well as information entered by the patient, such as changes in symptoms. Ultimately, such technology could be used to tailor medications to the individual.
Of course, these devices don’t work alone: Somewhere the data need to be interpreted, as in the VA’s telehealth program, by medical professionals. Eventually, though, as health sensors become commonplace in people’s homes and in the community, the onslaught of data will quickly overwhelm clinicians, so we will have to create smart systems that automatically interpret and act on the data they gather. These systems will be faster and more accurate than human clinicians at spotting anomalies and better at identifying those cases that require human consultation.
While all these technologies have exciting potential, the wireless revolution in health care does have a few obstacles in its path. There are regulatory hurdles, for starters. The technology of wireless medical devices is evolving at a much faster pace than our ability to contemplate all the potential consequences, good or bad. As a result, there is much confusion about what the technology might mean for patient safety, resulting in an understandable lag in regulatory guidance. To be sure, remote sensors linked to smart systems and adjustable therapies aren’t perfect yet. But far, far worse is the existing health care system in the United States, with its fragmented care, overburdened clinicians, lapses in following standard clinical guidelines, and perverse incentives that boost profits for some but diminish quality and efficiency of care for many. Frankly, wireless devices don’t have to be perfect to be better than what we have now.
People are also worried about privacy. They may fear that a device could be hacked or that data could be misused by employers or insurance companies. Yes, both could happen. But we can make it extremely unlikely. After all, many of us don’t even think twice about using mobile apps on our phones to check our bank accounts. You should be able to make your health care information at least as secure as your checking account.
We also need interoperability standards. At present, health care is a kind of Tower of Babel, with separate devices and databases containing bits and pieces of information about us but no single system accessible by patients, doctors, and caregivers that provides a complete and comprehensive picture of an individual’s health. What’s also missing is a universal interface for monitoring the functioning of a human body that’s as easy to understand as the gauges on a car’s dashboard. That is, in the same way a car’s dashboard shows us how much gas is left in the tank or if the engine is malfunctioning, we need an interface that clearly depicts health status and early warnings of disease or other trouble. This interface would bring together the data we gather about our vital signs, our medical conditions, and our varied and complex physiological responses to medications and then tell us what it all might mean.
Recent reforms in health care reimbursement policies made in U.S. legislation should help overcome these hurdles. And the creation of new models of care that cover a patient’s entire treatment at a fixed price—instead of charging each time a patient shows up at the doctor’s office—should offer incentives to use technologies that keep patients healthy and out of the hospital. The main thing that will drive adoption of these integrated wireless systems is the data that validate their cost-effectiveness; that will require studies and trials that go far beyond what the VA has done to date.
But I am convinced that we will get there. Eventually, we’ll tie together today’s trends—the expansion of tools for wirelessly monitoring and diagnosing disease, the increasing ability to remotely manage drugs and medical devices, and the growing understanding about how genetics affects susceptibilities to disease—with smart systems that learn as well as respond. And we will have a revolution in health care that changes society as dramatically as the Industrial Revolution once did.
This article originally appeared in print as “The Doctor Will See You Always.”